Note: The complete set of exhaustively detailed standards developed for this trial, can be accessed at this link: Basic scientific lab standards — Best practices for a replicable dietary intervention. That link is an ongoing work.
See also: Stealth Syndrome Study – Typical and Intervention Diets
To facilitate replicability the kitchen was operated in much the same manner as a bench lab.
This ad-free article is made possible by the financial support of the
Center for Research on Environmental Chemicals in Humans: a 501(c)(3) non-profit.
Please consider making a tax-deductible donation for continued biomedical research.
Food preparation took place in a 400-square-foot professional kitchen with stainless steel countertops and carbon-filtered water. A 1,200 cubic-feet/minute, four-centrifugal-fan exhaust hood was used over an eight-burner natural gas stove. Central air with HEPA filters ventilated the kitchen which was also equipped with two auxiliary standalone HEPA filter machines. Two electric ovens were used for baking. Additional efforts were also made to reduce other non-food exposures and confounding factors.
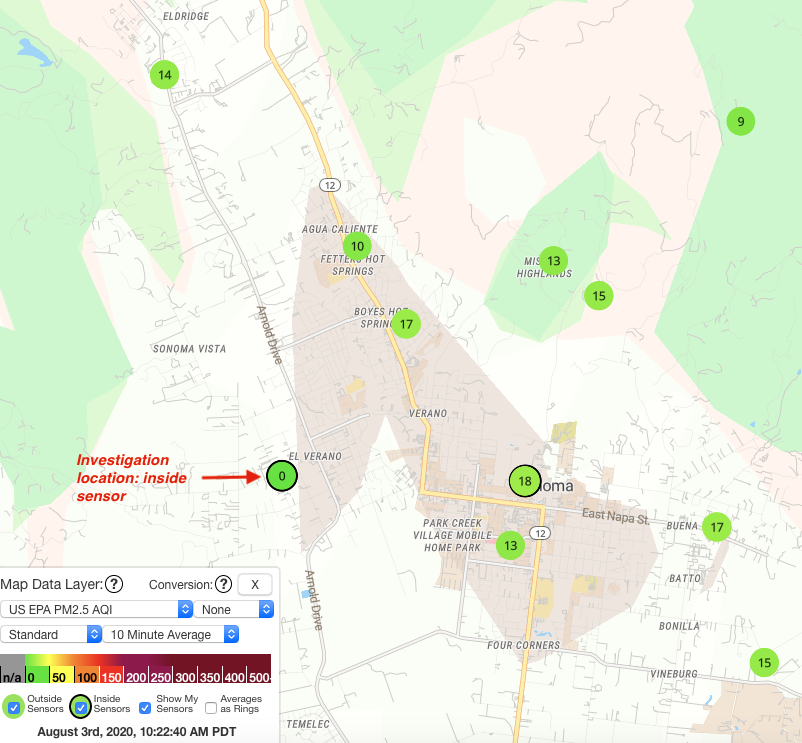
PM2.5 levels were monitored via sensors from PurpleAir.Com, one which monitored the kitchen air quality, as wel as numerous other outdoor sensors in a roughly five-mile radius.
All unacceptable materials were removed from the kitchen, including plastic and polymer items utensils, containers, and cookware with non-stick coatings. Only glass, stainless steel, aluminum foil, and tight grain maple cutting boards were allowed. Vinyl gloves were used in food preparation for sanitary control in both legs of the trial, but actual food contact with the gloves was minimal and incidental. 100% cotton dish towels were allowed, but paper towels could only be used for cleanup.
All measurements were by metric weight, and none by volume. This facilitated the kitchen’s staff’s accommodation from English to metric measurement because they could dispense with volumetric measurements which are problematic because of packing and granular particle size in solid items, and meniscus errors for liquid.
In converting recipes with English measurements, initial measurements for liquids was done in measuring cups with dual English/Metric gradations. Then, with a glass mixing bowl with dry ingredients already on a metric measuring scale, the liquid was added to the bowl and the metric weight recorded for the investigation data.
All main ingredients were measured to the nearest gram, but small-weight items such as spices, herbs and other seasonings and other items were measured to the nearest tenth of a gram. This is vital because those ingredients often have metabolic and other health effects in amounts out of proportion to their weight. For the same reasons, Investigators used spices they had grown for the purpose. Black pepper was obtained from an organic source. Peppercorns were rinsed, dried and ground with a grinder without plastic components. These measures were necessary because store-bought spices are among the most contaminated.
Items with known plastic contamination (such as micro-plastic contamination of table salt) were replaced where possible with reagents from Sigma-Aldrich.
Small kitchen-ready scales were obtained and calibrated using brass gram weights.
Culinary assistants were briefed on the measurement procedures and adapted very quickly.
All recipes and menus and a calendar of their serving dates and times were posted on a kitchen whiteboard directly above a dedicated counter surface on which recipes were places, and data recorded. Hand-written data was transferred to two master Excel spreadsheets for the Baseline and Intervention legs.